
African sleeping sickness is one of those scary diseases that seems kind of alien to anyone living in the Western world but which is a real threat to those living in sub-Sahara Africa, causing around 50,000 cases each year. The disease gets its name from the most recognisable symptom—a disruption of sleeping patterns after the parasite infects the brain. A recent paper published in PLoS One shed some light on how the parasite makes the treacherous journey from the blood to the brain. But why does a parasite spread by infected blood want to get into our head to start with?
Any infectious agent needs to have a plan of attack for dealing with the host’s immune system. Some microorganisms go along the route of actively switching off the immune response. Others hide from the immune cells that would otherwise kill them. The trypanosomes responsible for sleeping sickness use a less subtle but highly effective method to stay one step ahead of the immune system while circulating in the blood. The parasites are coated with ten million copies of the same protein which is recognised by the host, allowing the immune system to start clearing the infection. But, just as the host starts to get the upper hand, the parasite subtly changes this protein disguise so that they are no longer recognised by the immune system.
Without drugs, it is impossible for an infected person to deal with the infection and the disease is always fatal. But sleeping sickness has a fairly high rate of relapse even after treatment. One of the reasons for this could be that, at some point the parasite decides to make the trip from the blood and into the brain. Here, it is effectively protected from drug treatment, and can pass back into the blood system to continue the infection. An evolutionary explanation for this could be that some hosts are better at dealing with the infection than humans, and the brain represents a hiding place from the immune system.
This late stage of the disease—the brain stage—is not well understood. It takes weeks and months for the late symptoms including confusion, reduced coordination, daytime sleepiness, and insomnia at nigh to emerge, and the reasons for this remain elusive. One of the most interesting of these symptoms—the change in sleeping patterns—has an interesting explanation. Sleeping sickness is spread by the tsetse fly. The tsetse fly is one of the less pleasant creatures in the world and it has fairly disgusting table manners. It bites a hole in the skin, vomits up some of its last meal complete with any parasites along with agents to prevent the blood from clotting, and then feasts on the resulting blood pool. This isn’t particularly pleasant for the unfortunate owner of the blood. Therefore it helps if the meal happens to be asleep at the time of being fed on.
But how does the trypanosome succeed in altering a person’s sleeping patterns? It appears that this is a side effect of a signalling molecule used by trypanosomes to control cell density. When the parasite gets into the brain, it doesn’t want to cause extensive inflammation and get itself noticed. So it secretes a messaging molecule called PGD2 that tells neighbouring parasites to commit parasite-suicide for the good of the overall population. But PGD2 has also been shown to cause non-REM sleep when injected into the nervous system. So secreting PGD2 directly into the brain is useful to the parasite when a person is far more likely to be bitten by the tsetse fly if they fall asleep during the day.
So how does the parasite get into the brain in the first place? Our brains are cut off from our blood supply by the blood brain barrier—a barrier which actively prevents such things as parasites from making the trip out of our veins and into our central nervous system. In addition to the blood brain barrier, we also have a barrier between our blood and the colourless liquid in which our brains float, and it is across this barrier that the parasites make the journey into the brain. Hartwig Wolburg and coworkers demonstrated that this journey takes the parasite through hostile territory until it reaches it’s a position at the edge of the brain where it is protected from the immune system but can still reinvade the blood if it so chooses.
But the group responsible for this work also addressed the question of why the brain stage takes so long to emerge. Something interesting about their attempts to reproduce the brain infection in rats was that it proved impossible to simply inject parasites into the nervous system. Instead, the infection needed to take its usual course, beginning with the blood stage and progressed to the brain stage after some time. It appears that there are three forms of the parasite (shown in the figure at the top of the post)—a stumpy form which does not undergo the variation in its coat proteins and is killed by the immune system, an intermediate form which is responsible for the blood infection, and a slender form which can cross into the brain. How this slender form emerges and whether it really is required for brain infection remains to be determined, however.
Research such as this has the potential to help the development of future vaccines and drugs by teaching us more about how the infection progresses. The current treatment for the later brain stage of the disease involves an arsenic-derivative which kills one in twenty people and has been described as ‘fire in the veins’ by those unlucky enough to need to take it. Over the past few years, sleeping sickness has slowly been decreasing in numbers and it is hoped that in a decade this disease may finally be eliminated.
 |
| The three forms of trypansomes - slender, intermediate and stumpy. |
Without drugs, it is impossible for an infected person to deal with the infection and the disease is always fatal. But sleeping sickness has a fairly high rate of relapse even after treatment. One of the reasons for this could be that, at some point the parasite decides to make the trip from the blood and into the brain. Here, it is effectively protected from drug treatment, and can pass back into the blood system to continue the infection. An evolutionary explanation for this could be that some hosts are better at dealing with the infection than humans, and the brain represents a hiding place from the immune system.
 |
| Tsetse fly. Yuk. Image from Wikipedia |
But how does the trypanosome succeed in altering a person’s sleeping patterns? It appears that this is a side effect of a signalling molecule used by trypanosomes to control cell density. When the parasite gets into the brain, it doesn’t want to cause extensive inflammation and get itself noticed. So it secretes a messaging molecule called PGD2 that tells neighbouring parasites to commit parasite-suicide for the good of the overall population. But PGD2 has also been shown to cause non-REM sleep when injected into the nervous system. So secreting PGD2 directly into the brain is useful to the parasite when a person is far more likely to be bitten by the tsetse fly if they fall asleep during the day.
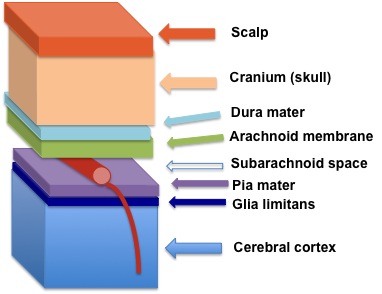 |
| The sleeping sickness parasite makes its way to reside between the Pia mater and Glia limitans at the edge of the blood. Image from: Wikipedia |
But the group responsible for this work also addressed the question of why the brain stage takes so long to emerge. Something interesting about their attempts to reproduce the brain infection in rats was that it proved impossible to simply inject parasites into the nervous system. Instead, the infection needed to take its usual course, beginning with the blood stage and progressed to the brain stage after some time. It appears that there are three forms of the parasite (shown in the figure at the top of the post)—a stumpy form which does not undergo the variation in its coat proteins and is killed by the immune system, an intermediate form which is responsible for the blood infection, and a slender form which can cross into the brain. How this slender form emerges and whether it really is required for brain infection remains to be determined, however.
Research such as this has the potential to help the development of future vaccines and drugs by teaching us more about how the infection progresses. The current treatment for the later brain stage of the disease involves an arsenic-derivative which kills one in twenty people and has been described as ‘fire in the veins’ by those unlucky enough to need to take it. Over the past few years, sleeping sickness has slowly been decreasing in numbers and it is hoped that in a decade this disease may finally be eliminated.










{kind=link}
{kind=link}